


If hospitalizations increase, will we wear masks again?
- May 7, 2022
- 0
Photo: Pixabay Were you hospitalized with covid or covid? Here is the question… Since the beginning of the pandemic, we have tried to base decision-making on data. While

9621 Agnes Crossing, Lake Suzanneview, New Mexico Island 84604-9295.
Photo: Pixabay Were you hospitalized with covid or covid? Here is the question… Since the beginning of the pandemic, we have tried to base decision-making on data. While


Were you hospitalized with covid or covid? Here is the question…
Since the beginning of the pandemic, we have tried to base decision-making on data. While there is room for differing interpretations, different data guide us on when and how intensively to implement or withdraw control measures.
Health administrations of almost all countries give us information about transmission, hospitalizations, admissions to the intensive care unit, deaths and vaccination rates. These data are generally presented by age groups and sometimes by vaccination status. Very relevant information for decision making, given the increased risk of developing severe covid in the elderly and the unvaccinated.
Contagion indicators were particularly useful in the first waves, when the population was not yet vaccinated or partially vaccinated, and there were particularly aggressive variants. They announced a few days in advance and with some certainty that they would be in the hospitals. It also made it possible to take action with minimal expectations regarding hospital data.
After the extraordinary vaccination campaign carried out in most European countries and the no less extraordinary wave of omicron, the situation changed. The population now has substantial immunological protection, most cases are mild, and the relationship between transmission and hospitalization has changed significantly.
These changes have caused many countries to lift restrictions, despite maintaining very high transmission numbers. And also to change their indicators. Infectors have lost interest, and decision-making is increasingly – and this makes sense – based on hospitalizations.
Hospitalization is close to the incidence of severe or moderate disease. Therefore, it is a much more important data for decision-making than the incidence of some cases that are mostly asymptomatic or barely symptomatic. And it is earlier than hospitalizations or deaths in intensive care.
The main problem in basing decision-making on hospitalization data is the definition of “hospitalization for covid-19” itself. A definition that refers to the presence of a positive result in a diagnostic test (PCR or antigens) for covid-19, not the cause or severity of the referral. Regardless of the patient’s condition and even if the reason for hospitalization is not coronavirus infection.
For this reason, the concept of health has begun to be used in health services. covid primary refer to cases where covid was the primary cause of hospitalization, and accidental covid Refers to applications that are positive for PCR or antigens, but the reason for hospitalization is not covid.
Obviously, primary covid means they’re entering for covid. Incidental covid means they entered with covid but not for covid.
Hospitals are seeing increasing numbers of covid cases, as most hospitals routinely test almost all hospitalized patients reasonably and transmission is still high. random This continues to inflate the government statistics of hospitalizations due to covid and complicates interpretation of the epidemiological situation.
Beyond anecdotal reports (from a hospital, a media report, etc.) there are very few studies on the incidence covid rate in hospitals. Also, few administrations have applied this differentiation, with the exception of a few special cases in the United States, Wales, and Canada.
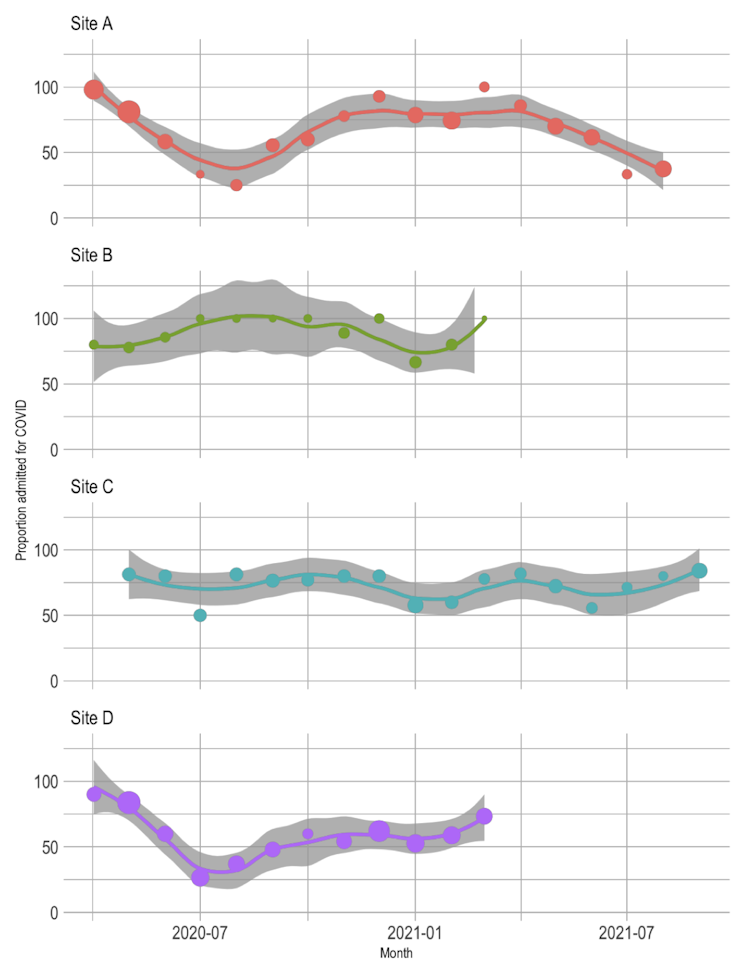
We know from some unexamined articles (preprint) the rate of primary hospitalizations (or vice versa, incidental) varies apparently over time and in different locations. For example, the rate of hospitalizations for primary covid in 4 US hospitals in different states during 2020-21 changed from 100% in the spring of 2020 to just 35% in the first fall of 2021. It also differed significantly between hospitals.
The available figures, reported from time to time by some countries where the Omicron variant predominates, are also variable. They depend on the transmission status in each region (in highly vaccinated populations, higher incidence of incidents, more transmission) depends on the operational definition of the disease. random adopted sources and sources of information.
At the end of April 2022, the Massachusetts Department of Public Health in the United States reported 31% of primary covid among patients hospitalized for covid, leaving two-thirds of hospitalizations incidental, which is a large number. Their very simple but possibly useful definition of primary covid was having received dexamethasone therapy, which can be considered a surrogate indicator of moderate or severe covid.
At the same time, the Welsh Department of Health estimated that only 19% of those hospitalized with covid were “actively treated”, equivalent to primary covid. In this case, the operational definition of “actively treated” is more complex and at the same time heterogeneous. In Canada, in February 2022, British Columbia reported 44% of incidental hospitalizations relative to total hospitalizations. with covid.
Other preprint Very recently, based on a single hospital in the Netherlands and patients infected with omycron only, it is estimated that covid was the reason (primary or contributing cause) of admission for 66% of PCR+ hospitalizations.
At this time of the epidemic, yes. It is not only useful, but also necessary for decision making. Conduction is growing and hospitalizations are increasing with transmission with and also, for covid. But the health response is very different depending on the ratio of each.
For example, if primary hospitalizations of the elderly or nursing homes are on the rise, an option to consider is to administer a 4th dose (second boost) of the vaccine. If the growth is mainly due to accidental hospitalizations, we can wait and try to give the second booster along with the flu shot. Perhaps with new or modified vaccines if they become available in the fall.
Other similar examples are the return of isolation, masks in confined spaces, sick leave of cases and contacts, etc. These are decisions that depend on the incidence of serious cases, not the incidence of cases. That is, primary hospitalizations.
However, relevant data are mixed with incidental hospitalizations (do not forget about patients). with covid) precludes an adequate interpretation of the seriousness of the situation. Incomplete information leads to speculative discussions and decisions that have a more political than scientific background. An example would be the positions taken in the current debate on the urgency of administering the 4th dose in the elderly and residential.
The accidental covid should not be trivialized. It is clear that it delayed planned admissions and required rescheduling of many hospital activities; this is something that is not always possible in such short periods of time. There are productivity losses and increased waiting. Where hospitalization cannot be postponed, it requires isolated rooms, the use of PPE, surveillance and other measures to prevent the spread of transmission to professionals and other patients. And sometimes, an incidental case at the time of presentation is complicated or complicates the primary disease leading up to the presentation.
By the way, the transmission should not be considered unfounded either. Many mild cases are just too much work for primary care and still have a lot to catch up on. And the increase in cases in general is always a residue from serious cases. Some measures should be taken to increase compliance with the Ministry’s own recommendations, even if it is just social communication.
Information systems should be useful in decision making. And when the situation changes and decisions to be made require new data or more precise data, they need to be changed. It has been important to distinguish between hospitalizations for primary or incidental covid since the middle of the sixth wave. And as hospitalizations increase, which we cannot interpret without too much uncertainty, this is also urgent.![]()
![]()
Salvador Peiró, Researcher, Health Services Research Area, FISABIO PUBLIC HEALTH, fisabio
This article was originally published on The Conversation. Read the original.
Source: El Nacional
Alice Smith is a seasoned journalist and writer for Div Bracket. She has a keen sense of what’s important and is always on top of the latest trends. Alice provides in-depth coverage of the most talked-about news stories, delivering insightful and thought-provoking articles that keep her readers informed and engaged.





