Are viral infections on the rise or are they just…
June 25, 2022
0
Photo: Pixabay The pandemic seems to have caused the unusual behavior of some common viruses. Especially those transmitted through the respiratory tract. There were almost no cases of
Photo: Pixabay
The pandemic seems to have caused the unusual behavior of some common viruses. Especially those transmitted through the respiratory tract.
There were almost no cases of flu in the 2020-2021 season. The 2021-2022 season started with low records, but unusually extended in the spring until it almost reached summer. Interestingly, a classic strain of the flu virus (Influenza B Yamagata) seems to have disappeared. Or at least not self-isolating in recent months.
Respiratory syncytial virus (RSV), the other “major” respiratory virus, has significantly reduced its incidence in 2020 and 2021. However, in the summer and outside of the usual season, he continued his strange behavior with epidemics.
Why did we humans lose our tails?
Fewer colds, more tuberculosis and monkeypox
Seasonal coronaviruses that cause the common cold have also reduced their presence in recent years. However, rhinoviruses that cause the common cold appear to have remained stable or even increased during the pandemic. It is a fact that makes us think that they can use different transmission routes from other respiratory viruses. We can even speculate that they are less responsive to mitigation measures and social distancing.
In the case of tuberculosis (a bacillus) worldwide, and after a decade of steady decline, deaths have risen to 1.5 million, even with a decrease in reported cases. But in some places, such as Washington State, very large outbreaks have been reported during the pandemic.
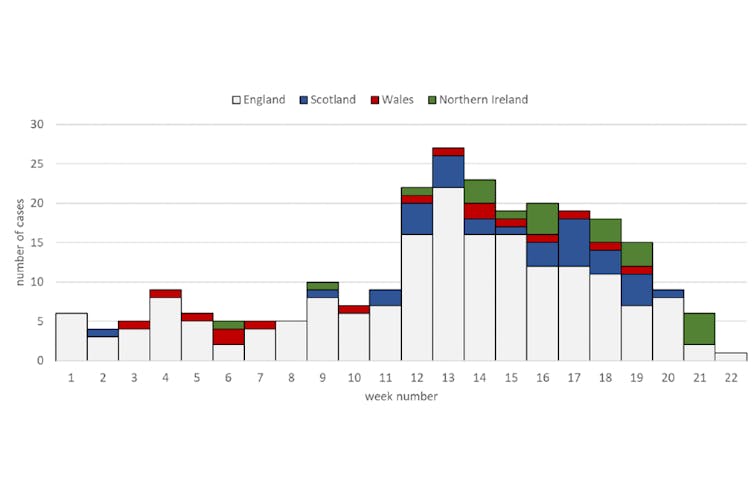
This year, beyond respiratory viruses, adenoviruses associated with outbreaks of acute childhood hepatitis of unknown origin surprised us (without clear causation). Fortunately, cases in the UK and Europe seem to have been declining in recent weeks with no clear explanation for the decline.
Cases of acute childhood hepatitis of unknown cause in the UK by week of admission. UK Health Security Agency, 2022
Frankly, we’ve been alarmed by the monkeypox virus, too. (monkey flower). Numerous outbreaks outside of its endemic area in West Africa and apparently unusual population groups and routes of transmission for this virus.
Geographical distribution of confirmed cases of monkeypox as of 15 June 2022. European Center for Disease Prevention and Control
What has changed with the pandemic?
There are several possible explanations for changes in virus behavior. First, the obvious is that many of the measures taken to reduce the transmission of SARS-CoV-2 also prevent transmission of other viruses.
Social distancing measures, masks, banning public events, limiting leisure and business travel (including intercontinental), reducing capacity and indoor ventilation, hand washing and some other measures seem sufficient to explain the reduction in respiratory infections. and contact transmission during the pandemic period.
Another explanation, derived from the previous and speculative, may be that microscopic competitors of SARS-CoV-2 have evolved to improve their adaptability to the selective pressure caused by mitigation measures. Evolutionarily, strains will be selected that can better compete with SARS-CoV-2.
It seems more plausible that our recent exposure to some viruses made us more susceptible when we discontinued mitigation measures. Or less exposure makes it harder for us to develop better immune responses after being infected and we see more severe cases of the same viruses. In that case, viruses wouldn’t change as much as we do.
A final explanation would simply be that our epidemiological surveillance systems (and our media and subjective perception of risk) have become hypersensitive to anything that looks like a virus. The more we stay vigilant, the more threats we detect. In fact, we will interpret things that did not seem so to us before as threats.
The more you look, the more you see
The recorded incidence of many health problems is highly sensitive to the type and intensity of screening activities. We’re talking about surveillance bias (surveillance bias) When these health problems are sought in different intensities across communities, over time, or according to the care setting and patient characteristics.
“Surveillance bias” causes us to find more cases when there isn’t much real variation in incidence as differences in detection intensity: the more you look, the more you see. The tuberculosis case is probably an example of the opposite: we reduced detection during the pandemic and now we are finding cases that we missed.
The impact of this bias has been discussed in other public health crises. For example, after the Chernobyl nuclear accident, an increase in thyroid cancer was detected in nearby areas. It was probably true, but the search for cancer after the accident is also likely to overestimate the extent of the increase.
There is also an increased incidence of Creutzfeldt-Jakob disease associated with a “mad cow” crisis (bovine spongiform encephalopathy); this is largely explained by the greater number of autopsies looking for this disease in older people.
A close relative of “surveillance bias” is the so-called “confirmation bias” (detection bias). It occurs when detection differs between population groups because exposure or risk is different.
For example, cases of monkeypox are more likely to be detected in men who have sex with men (MSM) than in heterosexuals. Simply put, some who experience the same symptoms will go to healthcare more than others. In addition, clinicians will look for the disease in people with MSM rather than heterosexuals.
Same explanation for all viruses?
It is possible that a single reason for the aforementioned does not explain the seeming strange behavior of very different viruses and different modes of transmission. In some cases, we will be more susceptible two years after exposure. In others, we will over-detect. In fact, both things at the same time, more or less.
In some cases, such as monkeypox or acute childhood hepatitis, it’s even possible that we’ve been detecting cases that have been lurking under the radar of our surveillance systems for some time, perhaps years.
And it is in this basket, in surveillance, that we need to put our efforts. Rather than bothering us with speculation about the “mental health” of microscopic beings, strengthening our epidemiological surveillance systems seems like the best way to address the future of our relationship with viruses.
Moreover, a future that seems uncertain and complex through climate change and globalization.
Salvador Peiró, researcher, Health Services research area, Fisabio Public Health, Physician.
This article was originally published on The Conversation. Read the original.
Independent journalism needs the support of its readers to keep going and have the disturbing stories at hand that they don’t want you to read. Today, with your support, we will continue to work hard for uncensored journalism!
Alice Smith is a seasoned journalist and writer for Div Bracket. She has a keen sense of what’s important and is always on top of the latest trends. Alice provides in-depth coverage of the most talked-about news stories, delivering insightful and thought-provoking articles that keep her readers informed and engaged.